Resident Corner: Before You Say No to Rural
You have already read the field report.
The itinerary that read like a geography lesson. The OR walked end-to-end in two minutes. The lake on a Tuesday afternoon in August. The number worth reading twice: 4.67 surgeons per 100,000 in rural America.
This is the operational companion. Not a case for going. Not against staying. The math and the scenarios you were never handed before interview season opened.
Two tools are embedded below. A third is linked at the close. Give it fifteen minutes before you decide.
Five rows. Two tracks. The same graduating surgeon.
Same physician. Two geographies.
One graduating surgeon. Two offers. Toggle between them.
The trap was never the rural offer. The trap was never being shown it existed.
Neither path is wrong. One of them was never shown to you. That is the only problem.
What rural surgery actually requires
Your assumption. Tap to see the field report.
01 The Backup System There is a protocol. Complex cases transfer. You are not the last line.
You are the last line. The helicopter waits for weather. The transfer protocol assumes a stabilized patient. You stabilize the patient.
02 Trauma Coverage Rural hospitals do stabilization. Complex trauma goes to a Level I center.
Level I is ninety minutes away on a clear night. Tonight it is not clear. You manage the hemorrhage, the airway, and the family. Simultaneously.
03 A Routine Appendectomy Lap appy. Forty-five minutes. Straightforward. Home by morning.
Perforated four days ago. They waited because the nearest ER was sixty miles. You open, you irrigate, you manage the ICU afterward. There is no fellow. There is no attending backup. There is you.
04 Surgical Scope Rural surgery means less. Simpler cases. A narrower scope than what you trained for.
You operate on pathology your academic colleagues subspecialized away from. The scope is not narrower. It is broader than anything your residency prepared you for.
05 The ICU at 4 AM The intensivist covers the unit. Surgery manages the surgical problem. That is how the system works.
There is no intensivist. Your post-op is febrile and your vent settings are drifting. You manage the pressors, adjust the rate, and call the family. That is also how the system works.
06 The Patient Relationship You will be one physician in a health system your patients navigate among many.
You will operate on the father of someone in your child's school. They will see you at the grocery store. You are not one of many physicians. You are the physician. That changes the work entirely.
Six scenarios. None of them in the residency curriculum. All of them on the schedule.
Six cases. All of them real. None of them in the curriculum.
If the toggle made you think and the scenarios did not turn you away, run one more check before you close the tab.
— enter your specialty and your state. Four data points come back: physician density against the national average, HPSA status and what it means for your Medicare billing, loan repayment eligibility by specialty, and non-compete enforceability in your state. All 50 states. Ten specialties. The numbers before the answer.
The gap between where surgeons are and where patients need them is going to keep widening. The only question is whether you looked at the math before you decided.
References & methodology
Physician workforce and rural shortage
AAMC. The Complexities of Physician Supply and Demand: Projections from 2021 to 2036. Association of American Medical Colleges, 2024. aamc.org
AAMC. 2024 State Physician Workforce Data Report. Association of American Medical Colleges, 2024. aamc.org/data-reports/workforce/data/state-physician-workforce-data-report
ACS. Rural Surgery Access and Surgical Workforce Shortage. Bulletin of the American College of Surgeons, 2024–2025. facs.org
HRSA National Center for Health Workforce Analysis. Health Workforce Projections. Health Resources and Services Administration, 2024. hrsa.gov/workforce/projections
HPSA designations and the 10% Medicare bonus
HRSA. Health Professional Shortage Area (HPSA) Finder. HRSA Data Warehouse, 2024. data.hrsa.gov/tools/shortage-area/hpsa-find
Centers for Medicare and Medicaid Services. Incentive Payments for Physicians in Health Professional Shortage Areas. CMS.gov, 2024. cms.gov/medicare/payment/fee-for-service-compliance-programs/health-professional-shortage-area-hpsa-bonus-payments
NHSC loan repayment
Health Resources and Services Administration. NHSC Loan Repayment Program. National Health Service Corps, 2024. nhsc.hrsa.gov/loan-repayment/nhsc-loan-repayment-program
Health Resources and Services Administration. NHSC Scholarship Program. National Health Service Corps, 2024. nhsc.hrsa.gov/scholarships/nhsc-scholarship-program
Non-compete enforceability by state
Federal Trade Commission. Non-Compete Clause Rule. FTC, 2024. ftc.gov/non-competes (Note: the federal rule faced legal challenge in 2024; state statutes govern enforceability in most jurisdictions. Verify current status in your state before relying on any non-compete summary.)
THE VAULT holds 12 tools for paid subscribers.
Built for residents who are about to make decisions that will follow them for a decade — and for attendings who wish someone had given them this at the start
FREE TOOLS
Four tools. No email. No catch. Run your numbers and keep them.
Built by a surgeon who wished these existed during training.
The W-2 True Cost Calculator
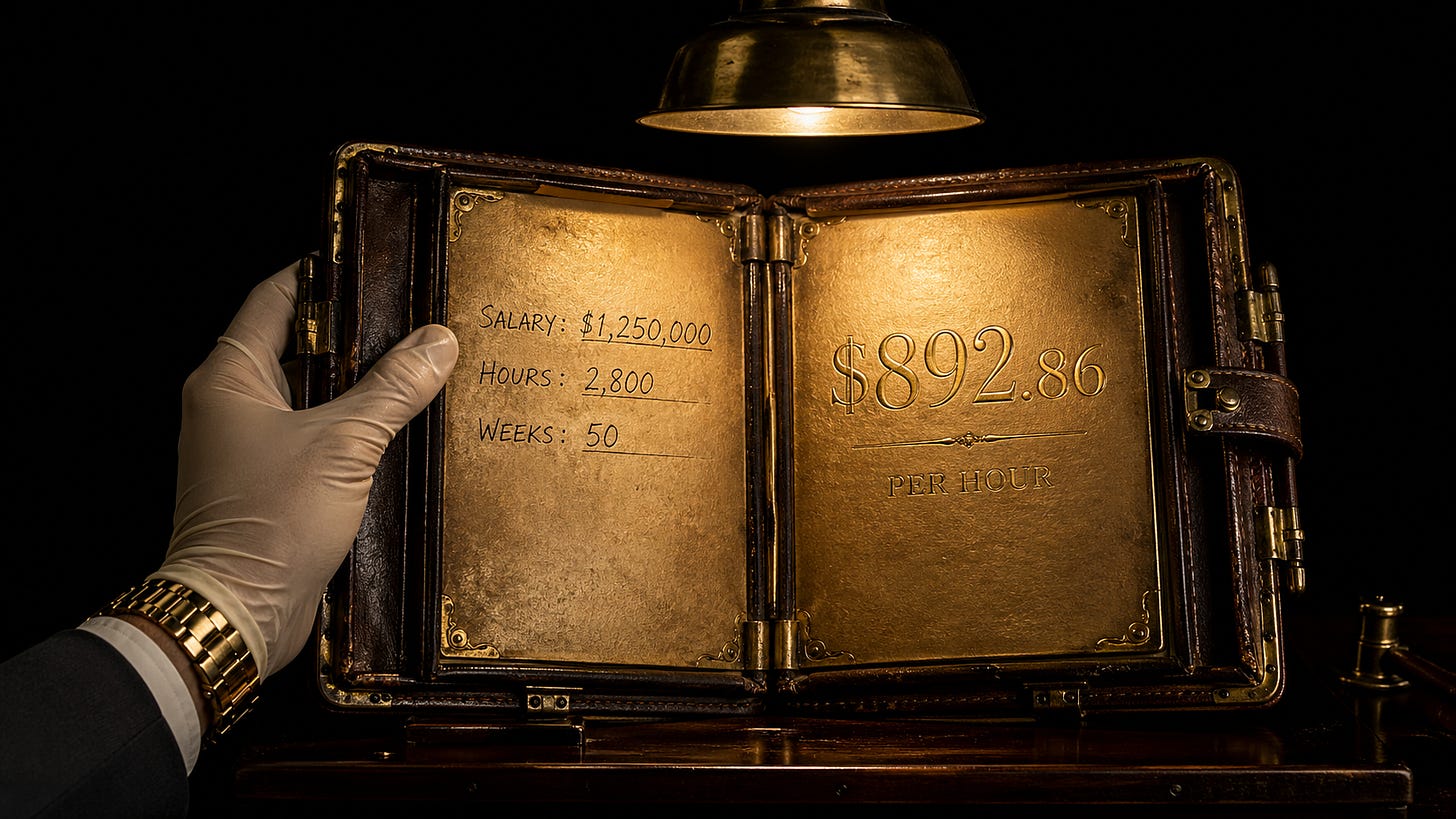
What is the real cost of an employed physician contract?
Most residents sign their first attending offer without running this number. Most attendings wish they had. Enter a salary, the hours, the weeks. The tool shows what that arrangement is actually worth — and what it costs you that the contract never mentions.
Run it on any offer before you sign it.
The Work Optional Timeline Calculator

The year work becomes optional is not fixed. It is a variable — and you control it.
Most residents never think about this number until they are ten years into an arrangement that was never designed to give it to them. Enter what you will earn, what you will save, what you will spend. The tool returns one number.
The earlier you run it, the more it changes.
The Five Dials Diagnostic

Five dimensions. Twenty questions. One archetype.
For attendings: know where you actually stand before you decide where to go.
For residents: know where you want to go before someone else decides for you.
Most physicians discover their Five Dials score after signing a contract that scores them a zero on autonomy. This takes four minutes. Run it before the offers come.
FREE REFERENCE
The IPM Glossary
21 terms physicians need to know — contract language, business vocabulary, the framework. One page. Built because nobody handed us this at the start.
Work optional. Life intentional.
— Golden Scalpel
Nothing here is financial, legal, or medical advice. Golden Scalpel is an independent media publication. Always consult a qualified professional before making major decisions. This is perspective, not prescription.